Chronic obstructive pulmonary disease (COPD): Everything there is to know
What is COPD?
Definition
Chronic obstructive pulmonary disease (or COPD) is a group of chronic inflammatory diseases affecting the airways (especially the bronchi). It leads to permanent and progressive obstruction of the airways, causing breathing difficulties and is associated with a destruction of the lung parenchyma called emphysema.
It is mainly caused by smoking (active or secondhand) and evolves in several stages. It starts with simple chronic bronchitis, which turns into chronic obstructive bronchitis and ends with emphysema (i.e. the destruction of the lining of the pulmonary alveoli).
Gas exchange is then disrupted, resulting in damage to the respiratory muscles associated with respiratory failure, pulmonary hypertension, and systemic (body-wide) effects such as osteoporosis and depression.
How common is COPD?
COPD is a common, though often under-diagnosed, condition. According to the WHO (World Health Organization), 251 million people had COPD in 2016 and it could become the third leading cause of death worldwide by 2030.
In the US, it affects more thank 16.4 million people, but many more may be undiagnosed.
Historically, COPD affected men more frequently than women, but today it affects almost as many men as women. This is mainly due to an increase in smoking among women.
Mortality of COPD is high (estimated to be more than 140,000 deaths per year, or the equivalent of 1 death every 4 minutes).
Symptoms and complications of COPD
COPD is a slow-developing and insidious disease. As such, it is often underestimated. Its main symptoms are coughing, excess phlegm or mucus and shortness of breath, to a greater or lesser extent depending on the stage of the disease. These symptoms generally appear around 40-50 years of age.
According to the mMRC (Modified Medical Research Council) scale, an evaluatory tool used in diagnosis, there are 5 grades of breathlessness, a defining symptom of COPD:
- Grade 0: breathlessness only with strenuous exercise;
- Grade 1: breathlessness when hurrying on level ground or walking on a slight incline;
- Grade 2: breathlessness requiring one to walk slower than someone of the same age on level ground, or having to stop for breath when walking at own pace on level ground;
- Grade 3: having to stop for breath after walking 100 yards or after a few minutes on level ground;
- Grade 4: too breathless to leave the house or breathlessness while dressing.
These different phases in the evolution of the disease may be interspersed with periods of exacerbation: i.e. aggravation of cough, sputum and in particular, breathlessness. They may require emergency medical care or even hospitalization and may lead to death (superinfection, respiratory failure, etc.).
In addition, COPD patients very often have many co-morbidities (other conditions related to the primary illness). These can be cardiac (e.g. high blood pressure), metabolic (e.g. malnutrition or weight loss), muscular (e.g. muscle weakening), skeletal (e.g. osteoporosis) and neurological (e.g. anxiety, depression). These co-morbidities are thought to be associated with the inflammatory processes involved in COPD: this is known as oxidative stress (aggression of the body's cells by oxidizing molecules).
Causes and risk factors of COPD
Tobacco (active or passive exposure, including second-hand smoke in utero) is the leading risk factor and is thought to be responsible for 80% of COPD cases.
Other risk factors also come into play, especially in the triggering and aggravation of symptoms:
- Indoor air pollution, such as the use of fuels for cooking and heating (carbon monoxide or CO), but also the presence of mold;
- Outdoor air pollution (carbon monoxide, volatile organic compounds, ozone, nitrogen dioxide, fine particles, etc.);
- Occupational exposure to dust (silica, coal) and chemicals (vapors, irritants and fumes);
- Frequent lower respiratory tract infections in childhood (bronchitis, bronchiolitis, influenza and pneumonia);
- The use of inhalants such as cannabis.
Diagnosing COPD
A COPD diagnosis can be made in a smoker if:
- One or more of the following signs is present: daily cough and excess mucus or phlegm production, (> 2-3 months per year), persistent progressive dyspnea (shortness of breath), appearing or worsening with exertion or after bronchitis;
- The person is exposed (in the workplace or at home) to toxins or irritants, including tobacco;
- The patient’s forced expiratory volume (FEV-1) is decreased.
There is no single test for COPD, so doctors diagnose it based on symptoms, a physical exam, and the results of a few diagnostic tests. One such test is pulmonary function testing (PFT). This is carried out using a spirometer: an electronic device with a mouthpiece into which the patient breathes. Spirometry measures the amount (volume) and/or speed (flow) of air that can be inhaled and exhaled and helps to identify the obstructive ventilation disorder that is virtually irreversible in the case of COPD.
The following is noted:
- A lower-than-normal in FEV-1 (forced expiratory volume in one second): it has a prognostic value and makes it possible to estimate the disease's progression;
- A FEV1/FVC* ratio (also called the Tiffeneau-Pinelli index) < 70%
* FVC (Forced vital capacity) is the maximum volume of air a person can expel from the lungs after full inspiration.
The PFT is complemented by a plethysmograph, which measures the functional residual capacity (FRC) of the lungs - the volume of air in the lungs when the respiration muscles are relaxed - as well as total lung capacity. In the case of emphysema, air is trapped in the lungs, inducing pulmonary distension (increase in total lung capacity).
A chest X-ray must also be taken: it often shows thoracic distension and capillary rarefaction, which is a sign of emphysema. It also allows for the detection of conditions that are common in smokers; lung cancer or cardiac abnormalities.
Doctors may use the Global Initiative for Chronic Obstructive Lung Disease (GOLD) grading system to describe the severity of COPD. The original version of this system relied only on the results of the forced expiratory volume (FEV-1) test to class COPD into four stages:
- Stage 1: mild, FEV-1 >80%
- Stage 2: moderate, FEV-1 50-79%
- Stage 3: severe, FEV-1 30-49%
- Stage 4: very severe, FEV-1 <30%
In recent years, the GOLD system has been updated to establish the grade of a patient’s COPD based on their symptoms, the number of exacerbations experienced, the number of hospitalizations because of COPD and the test results mentioned above. Stages are now referred to as grades and range from GOLD 1 (mild) to Gold 4 (very severe).
COPD patients may also be given a group classification according to symptoms, exacerbation frequency, and severity:
- Group A (low risk, less symptoms): Stage 1 or 2, 1 or fewer exacerbations per year, no hospitalizations, mMRC grade 0-1 or COPD Assessment Test (CAT) <10;
- Group B (low risk, more symptoms):Stage 1 or 2, 1 or fewer exacerbations per year, no hospitalizations, mMRC 2 or higher or CAT ≥10
- Group C (high risk, less symptoms): Stage 3 or 4, 2 or more exacerbations per year, 1 or more exacerbation with hospitalization, mMRC 0-1 or CAT <10;
- Group D (high risk, more symptoms): Stage 3 or 4, 2 or more exacerbations per year, 1 or more exacerbations with hospitalization, mMRC 2 or higher or CAT ≥10
Treatments for COPD
The goal of COPD treatment is to prevent the progression of the disease. They also provide relief from symptoms, improve exercise tolerance and quality of life, and prevent and treat complications and exacerbations. In this way, they help to reduce mortality caused by COPD.
Common preventive measures at all stages of COPD
The first step in treating COPD is to reduce or stop the risk factors. Quitting smoking is paramount and should be started as soon as possible (this is the main treatment for the decline in FEV-1).
The evaluation of one's tobacco addiction can be assessed using the Fagerstrom Test For Nicotine Dependence (FTND). Pharmacological treatments are also available: nicotine substitutes have many different galenic forms (tablets, gums, lozenges, patches, inhalers, nasal sprays, etc.) and are covered by the NHS. If anxio-depressive factors and addictive behavior are associated with tobacco consumption, the use of medicines such as varenicline (Champix®) or bupropion (Zyban®) may be considered. Cognitive behavioral therapy (CBT) or hypnosis is also an option. Finally, psychological support can be very useful in helping people to stop smoking.
In addition, it is important to prevent the occurrence of bouts of infection. To do this, it is important to clean one's hands regularly and carefully, to have good oral hygiene, to rinse the nasal cavities, and to clean and disinfect one's environment and equipment on a regular basis. Flu vaccination is recommended every year and pneumococcal vaccination every 5 years.
Preventing exposure to pollutants, toxins and irritants, whether occupational or not (silica, coal dust, plant dust, mold, etc.) is also part of the preventive measures common to all stages of the disease. It is possible to seek the advice of the occupational physician for this purpose. It is also important to regularly ventilate one's interior (especially after the use of chemical products during cleaning).
Treatment of COPD symptoms
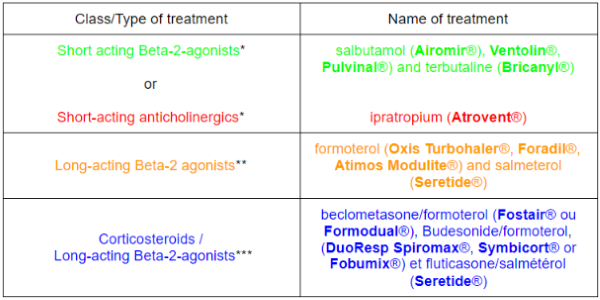
In addition to these preventive measures, medication is prescribed to treat COPD symptoms. This differs according to the stage of the disease and in most cases the following is recommended:
- Inhalation of a short acting bronchodilator* when needed, at any stage of the disease;
- Inhalation twice a day of a long-acting bronchodilator**, from stage 2 (moderate) to stage 4 (very severe);
- Inhalation twice a day of a fixed-dose combination of corticosteroids with a long-acting bronchodilator***, from stage 3 (severe) to stage 4 (very severe).
Finally, long-term oxygen therapy should be considered if stage 4 (very severe) and chronic respiratory failure (CRF) are present.
It should be noted that there are also ultra-long-acting Beta-2-agonists (which cause bronchial dilatation), such as indacaterol (Onbrez®) and olodaterol (Striverdi Respimat®), and anticholinergics, such as glycopyrronium (Seebri®), umeclidinium (Incruse Ellipta®) and tiotropium (Spiriva®), which are very long-acting. They are administered once a day.
A Beta-2-agonist can also be associated with an anticholinergic: very long-acting agents such as umeclidinium associated with vilanterol (Anoro Ellipta®), glycopyrronium associated with indacaterol (Ultibro®) and tiotropium associated with olodaterol (Spiolto Respimat®).
Finally, there is also an ultra-long-acting combination of Beta-2-agonists and corticosteroids, such as vilanterol combined with fluticasone (Relvar Ellipta®) to be used once a day.
In addition, pulmonary rehabilitation aims to reduce breathlessness, decrease disability, increase autonomy and improve quality of life. It consists of re-training for exertion through breathing and muscular exercises (stationary bicycle, treadmill or rowing machine) and pulmonary physical therapy aimed at improving bronchial drainage. It can take place in a hospital environment, in specialized centers or at home.
In very severe cases of the disease (partial pressure of oxygen PaO2 ≤ 55 mmHg or PaO2 ≤ 60 mmHg combined with right-sided heart failure, pulmonary hypertension, an increase in the number of red blood cells (polycythemia), or a decrease in oxygen saturation at night called nocturnal hypoxemia), long-term oxygen therapy (> 3 months) at a rate of at least 15h/d may be considered. Oxygen therapy can improve the patient's quality of life and reduces the number of exacerbations, but does not change the prognosis of COPD. It involves the patient breathing in air that is richer in oxygen (O2) than the ambient air. The aim is to maintain:
- A PaO2 > 60 mmHg (Normal values are between 80 and 100 mmHg);
- An arterial oxygen saturation SaO2 ≥ 90%. The normal value is > 95%.
Mucoactive agents (mucolytics or expectorants) should not be used. These drugs increase the volume of bronchial secretions (mucus) and may increase bronchial obstruction if the patient has difficulty expectorating.
Likewise, cough suppressants are not indicated for COPD, as on the contrary the cough must be observed and physical therapy techniques must be used to drain bronchial hypersecretion.
Management of COPD exacerbations
A COPD exacerbation is a worsening of symptoms leading the patient to seek emergency medical attention. It is most often related to an infection in the airways.
In the absence of aggravating criteria (dyspnea at rest, cyanosis, disorders of consciousness), care is performed on an outpatient basis (lasting only a few hours without hospitalization), with recourse to the primary care physician or the pulmonologist, and then the treatment is adapted (with an increase, if necessary, in the bronchodilating treatment).
Antibiotic therapy and physical therapy for bronchial drainage may be used.
In case of severe symptoms (with FEV-1 < 30% and partial pressure of oxygen or PaO2 < 60 mmHg) or secondary aggravation, treatment should be carried out in a hospital as a matter of urgency.
Oxygen therapy to achieve an oxygen saturation or SaO2 > 90%, a 7 to 14 day course of antibiotics, bronchodilators in a nebulizer and physical therapy for bronchial drainage are implemented. Corticosteroids are not systemically administered.
Living with COPD
Monitoring and care
Clinical monitoring and the frequency and organization of follow-up between the general practitioner, pulmonologist and other health professionals depend on the grade of the disease and the associated comorbidities (undernutrition, anxiety, depression, cardiovascular disease, etc.).
In grades 1 and 2, the primary care physician (PCP) should be consulted once or twice a year and a pulmonologist's opinion may be sought if necessary.
For grade 3, the PCP should be consulted every 3 months and the pulmonologist once a year.
For grade 4 a monthly visit to the PCP and a visit to the pulmonologist every 6 months is recommended. Of course, these visits can be adapted to the patient’s needs.
A clinical evaluation is necessary at all stages of COPD (smoking, exposure to toxic substances, tolerance and compliance with treatments, techniques for using inhalers and nebulizers, etc.). Consulting other specialists (physical therapist, cardiologist, psychologist, nutritionist, etc.) can also be complementary to COPD treatment. If the patient has not stopped smoking, it is recommended that he or she consult a stop smoking adviser or visit a stop smoking clinic.
From grade 2 onwards, a program monitoring pulmonary rehabilitation is put in place.
From grades 3 and 4, the need for long-term oxygen therapy (LTOT) and/or non-invasive ventilation (NIV) is assessed.
An overall assessment is then carried out, taking into account the needs and expectations of the patient, estimating the dyspnea score* and a 6-minute walking test by the pulmonologist or rehab therapist.
*The mMRC scale allows to estimate the dyspnea score equal to:
- 0 if the patient is breathless only with strenuous exercise;
- 1 if the patient is breathless when hurrying on level ground or walking on a slight incline;
- 2 if the patient has to walk slower than someone of the same age on level ground or has to stop for breath when walking at his or her own pace on level ground;
- 3 if the patient has to stop for breath after walking 100 yards or after a few minutes on level ground;
- 4 if the patient is too breathless to leave the house.
The rhythm of the pulmonary function tests (PFT) will be adapted to the patient's state of health. A blood gas test should also be done if there is a worsening of COPD. From stage 3 onwards, a complete blood count (CBC), including an assessment of the number of platelets, should be performed once a year to assess the presence of polycythemia (high red blood cell count) or anemia (insufficient red blood cells, or hemoglobin) or undernutrition.
Monitoring treatment
In order to monitor the effectiveness of treatment, the frequency, intensity and duration of exacerbations (increased coughing, sputum turning greenish and shortness of breath) should be assessed. They are largely caused by infection but are also linked to pollution or right-sided heart failure.
In addition, clinical monitoring is necessary to prevent the various undesirable effects of inhaled medicines:
- Beta-2-agonists can cause tachycardia and tremors;
- Anticholinergics can cause dry mouth, tachycardia, palpitations and in rare cases, prostate symptoms. They may also contribute to or aggravate glaucoma. It is therefore important to be careful of getting any spray in the eyes and to wash one's hands after using the medication;
- Inhaled corticosteroids can cause oral thrush and a hoarse voice: it is important to rinse out the mouth after use;
- Oxygen therapy may cause dry nose, mouth and eyes: use of a humidifier is recommended. Moreover, this device is very flammable: it is therefore strictly prohibited to smoke or to be near open flames (a fireplace, for example). It is also important to check the mask for leaks and to avoid applying ointment or cream to the face;
- Finally, benzodiazepines (Lexomil®, Xanax®, Valium®) are contraindicated for the treatment of COPD as they can increase respiratory problems.
Therapeutic patient education (TPE)
The aim of therapeutic patient education is to make the patient more independent, improve his or her quality of life and reduce the occurrence of exacerbations. It is an integral part of pulmonary rehabilitation and essential at all stages of the disease.
Its objectives are a better understanding by the patient of his or her disease and treatments, and thus a better adherence to treatment in order to slow down the progression of the disease. Thanks to ETP, the patient becomes aware of the possible side effects of his or her treatments but also of the means to avoid them.
He or she knows how to recognize the symptoms of an exacerbation at an early stage (increased dyspnea, purulent sputum and coughing) and how to remedy them.
In addition, therapeutic education enables the patient to understand the importance of quitting smoking, to recognize his or her dependence and to learn about the many treatments and support structures available to facilitate this cessation.
TPE helps to recall and implement preventive measures such as: exposure to pollutants and toxins, flu vaccination (annual) and pneumococcal vaccination (every 5 years).
Finally, therapeutic education allows patients to learn inhalation and bronchial decongestion techniques to ensure the correct use of medical devices associated with inhaled treatments.
Physical activity and nutrition
To slow down the evolution of COPD and limit its impact on quality of life, it is recommended to adopt a healthy lifestyle.
Dietary measures are important in order to avoid weight loss or even undernutrition which could aggravate the disease. Being overweight, on the other hand, can cause shortness of breath.
A balanced diet, rich in proteins, fiber and antioxidants and low in fat, salt (especially with the intake of corticoids) and sugar, is recommended and must be adapted to one's nutritional needs.
Physical activity (PA) is an essential component of pulmonary rehabilitation and helps to slow down the progression of the disease as a complement to drug treatment. In particular, it reduces fatigue and anxiety and increases muscle performance and quality of life. It also improves cardiovascular capacity, increases muscle oxygenation and exercise tolerance.
It is advisable to make an appointment in advance with one's primary care doctor to determine the most suitable physical activity for one's personal situation. An initial medical assessment may also be necessary, especially for patients with cardiovascular risk factors.
There are different types of physical exercises:
- Endurance exercises: it reduces breathing rate, heart rate, dyspnea and the production of lactate in the blood.
- Strengthening exercises: it improves muscular strength (especially of the lower limbs).
The ideal would be to combine these 2 types of physical activities.
The Centers for Disease Control and the American College of Sports Medicine recommend at least 150 minutes of light to moderate- intensity aerobic activity per week, including activities like brisk walking, walking up stairs, dancing, or gardening. This can be divided into smaller periods, such as about 20 minutes per day, or 30 minutes 5 days a week. Muscular strengthening exercises (using weights, elastic bands or other equipment) can be performed 2 to 3 non consecutive days a week and exercises to increase flexibility (stretching) can be done 2 to 3 days a week or even daily. Naturally, these recommendations must be adapted according to each person's abilities.
At the stage of respiratory failure, although exercising a sport is difficult, it is still essential to maintain the muscles. The physical therapist is in charge of this muscular training, which can be combined with respiratory therapy, and a minimum of daily physical activity must be maintained.
In conclusion, COPD is a chronic respiratory disease that cannot be cured, but appropriate care (early diagnosis, healthy lifestyle, therapeutic education, preventive measures and drug treatment) can improve patients' daily lives. Quitting smoking is essential to prevent the disease from worsening.
Sources:
COPD, World Health Organization
Chronic obstructive pulmonary disease in adults, National Institute for Health and Care Excellence
Learn About COPD, American Lung Association
COPD, Center for Disease Control and Prevention
Arterial Blood Gases, University of Michigan
Pulmonary Function Tests, John Hopkins Medicine
Pocket Guide to COPD Diagnosis, Management, and Prevention, Global Initiative for Chronic Obstructive Lung Disease
The MRC Breathlessness scale, Occupational Medicine
COPD assessment: I, II, III, IV and/or A, B, C, D, European Respiratory Journal
The ABCD of GOLD made clear, European Respiratory Journal
COPD, Mayo Clinic
Chronic obstructive pulmonary disease (COPD), CDC
Managing Your COPD Medications, American Lung Association
Fagerstrom Test for Nicotine Dependence, American Association for Respiratory Care
GOLD Classification for chronic obstructive pulmonary disease (COPD), Medscape
Physical Activity and COPD
Exercising with Chronic Obstructive Pulmonary Disease (COPD), American College of Sports Medicine
Physical Activity Guidelines for Americans 2nd Edition, Department of Health & Human Services
Published Nov 4, 2020


